Performances
- Puncture (K3 vs. pencil)
- Pencil point needles cause puncture resistance that is up to three times greater than the resistance encountered by K-3 lancet point needles.
This resistance affects the skin and tissues when the needle passes through.
This is why it is recommended that an introducer is used with the non-cutting pencil point needle.
On the other hand, the resistance may enable the anesthetist to perceive more distinctively the transit through the arachnoid mater, therefore decreasing the risk of nerve puncture.
- Puncture cuts (Cutting vs. non-cutting)
- Several studies explain why a non-cutting point needle is less likely to cause PDPH.
One of the theories is that the cutting point needle makes a sharp crescent-shaped cut in the arachnoid mater, while the non-cutting point needle makes an opening in the arachnoid mater comparable to a pushed-open clam shell.
We have confirmed very similar opening shapes in an in-house experiment using polyamide films.
The sharp crescent-shaped cut took a long time to adhere while the blunt clam shell opening took less time to adhere, despite its large opening surface.
Unisis Pencil Point 25G Unisis K-3 Lancet point 25G 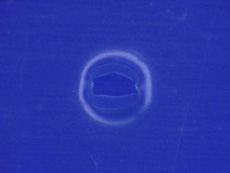

- Successive images of CSF leak simulation
- Using a measuring cylinder as the spinal cord, red-colored water as CSF, and the polyethylene film as the arachnoid mater, we observed the water leak after needle puncture of the film.
The puncture was considered more invasive when more water leak was observed following removal of the needle.
The red water leak stopped more quickly with the non-cutting needle than with the cutting needle, suggesting a more prompt CSF leak control is possible with a non-cutting needle.
Unisis Pencil Point 25G Unisis K-3 Lancet point 25G Immediately after removal 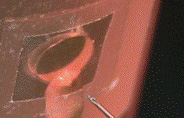

Presence/absence of countinuous leakage 
